
Congenital Hip Dislocation: A Comprehensive Guide (Developmental Dysplasia of the Hip – DDH)
What It Is
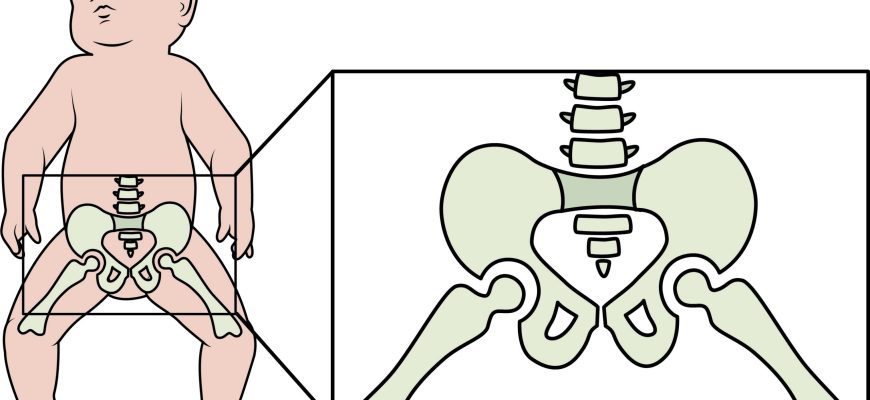
Congenital hip dislocation, now more accurately referred to as Developmental Dysplasia of the Hip (DDH), is a condition where a baby’s hip joint does not form properly. The term “congenital” means present at birth, but DDH can both develop before birth or in the weeks and months after birth. It encompasses a spectrum of abnormalities: the hip socket (acetabulum) may be too shallow; the ball (femoral head) may be loose within the socket (subluxatable); or it may be completely dislocated.
Types / Spectrum of DDH
DDH is not a single condition but a range of hip instability:
- Acetabular Dysplasia: The hip socket is shallow but the femoral head remains in place.
- Subluxatable Hip: The femoral head is loose within the socket and can be partially displaced with a physical exam.
- Dislocatable Hip: The femoral head is within the socket at rest but can be completely pushed out of the socket with a manual exam.
- Dislocated Hip: The femoral head is not in contact with the socket at rest. This can be:
- Reducible: The hip can be manually put back into the socket.
- Irreducible (Teratologic Dislocation): The hip is permanently dislocated, often associated with neuromuscular conditions like spina bifida or arthrogryposis. This is rare and more severe.
Symptoms
Symptoms can be subtle and are often detected by a pediatrician during screening. Parents might notice:
In Infants:
- Asymmetrical thigh or buttock folds: The skin folds on the thighs or under the buttocks may not match.
- Limited Range of Motion: One hip may not abduct (spread open) as widely as the other.
- Positive “Barlow” or “Ortolani” Sign: A clunk or click felt when the hip is manipulated (this is a clinical sign assessed by a doctor, not a parent).
- Apparent Leg Length Discrepancy: The leg on the dislocated side may appear shorter.
In Older Babies and Children:
- Limping when the child begins to walk.
- Walking on toes on one foot.
- A waddling “duck-like” gait if both hips are affected.
- Asymmetric crawling.
- Increased lumbar lordosis (swayback) in bilateral cases.
Diagnosis
- Newborn Physical Exam: The cornerstone of diagnosis. All newborns are screened for DDH using the Barlow (tests for a dislocatable hip) and Ortolani (tests for reducing a dislocated hip) maneuvers.
- Imaging:
- Ultrasound: The primary imaging tool for infants under 6 months old, as their hip bones are still mostly cartilage. It provides a dynamic view of the hip’s position and structure.
- X-ray: Becomes more useful after 4-6 months of age when the femoral head begins to ossify (turn to bone). It is used to confirm diagnosis and monitor treatment progress in older infants and children.
Prevention
There is no sure way to prevent DDH, as genetics and fetal position play a large role. However, certain practices can help promote healthy hip development in newborns:
- Hip-Healthy Swaddling: Always swaddle a baby with the legs able to bend up and out. Tight swaddling with legs straight and pressed together is a risk factor and should be avoided. The International Hip Dysplasia Institute promotes “hip-healthy swaddling.”
- Carrying in a Sling/Carrier: Use carriers that support the thigh and allow the hips to be in a “M” position (knees higher than bottom).
- Avoid prolonged positioning that holds the legs straight and together.
Treatment
Treatment is highly dependent on the child’s age and the severity of the dysplasia. The goal is to center the femoral head in the socket to allow for normal development.
- Newborns to 6 months: The Pavlik Harness is the standard first-line treatment. It is a soft brace that holds the baby’s hips in a flexed and abducted (“frog-legged”) position, allowing the hip to stabilize and the socket to deepen. It is typically worn full-time for 6-12 weeks.
- 6-18 months / Failed Harness: If the harness fails or the child is older, closed reduction under anesthesia is performed. The doctor manually positions the hip correctly, and then a spica cast is applied to hold it in place for several months.
- Older Children (18+ months) and Adults: DDH diagnosed later in life often requires more extensive treatment to correct the developed deformity and arthritis.
Types of Surgery
Surgery is required for older children or when closed methods fail.
- Closed Reduction with Spica Casting: Often considered a procedure rather than surgery, as no incision is made.
- Open Reduction: A surgical procedure where an incision is made to remove obstacles that prevent the hip from seating properly (e.g., tight tendons, tissue). The hip is then placed in the socket and a spica cast is applied.
- Osteotomy: This is a bone-cutting procedure to realign the hip joint. It may be performed on the femur (femoral osteotomy), the pelvis (e.g., Salter, Pemberton, Dega osteotomy), or both to correct the abnormal shape of the bones and provide better coverage of the femoral head.
Prognosis
The prognosis is excellent when DDH is diagnosed and treated early.
- Infants treated with a Pavlik harness have a success rate of over 90%.
- The later the diagnosis, the more complex the treatment and the higher the risk of long-term complications.
- Untreated DDH leads to premature wear-and-tear arthritis, chronic pain, a limp, and leg length discrepancy in adulthood.
- Even with successful treatment, some children may have a slightly increased risk of developing arthritis later in life compared to the general population.
Warning Signs & When to See a Doctor
All babies are screened at birth and at well-baby checkups. See a pediatrician or pediatric orthopedist if you notice:
- Asymmetrical skin folds on your infant’s thighs.
- A “clicking” or “clunking” sound with diaper changes.
- Limited range of motion in one hip.
- One leg appears longer than the other.
- A limp or waddling gait when your child begins to walk.






