
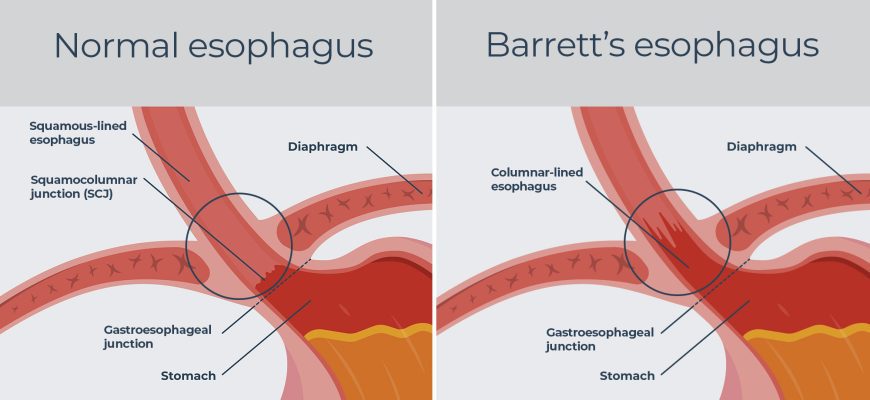
Barrett’s esophagus is a precancerous condition where the normal lining of the esophagus is replaced by intestinal-like tissue due to chronic acid reflux (GERD). It increases the risk of esophageal adenocarcinoma, a serious type of cancer.
Etiology (Causes & Risk Factors)
Primary Cause:
✔ Chronic GERD (long-term acid reflux damages esophageal cells)
Other Risk Factors:
- Age (>50 years)
- Male gender (3-5x more common in men)
- Obesity (especially abdominal fat)
- White ethnicity
- Smoking & alcohol use
- Family history of Barrett’s or esophageal cancer
Types
- Non-dysplastic Barrett’s esophagus – Abnormal cells without precancerous changes
- Low-grade dysplasia – Early precancerous changes
- High-grade dysplasia – Advanced precancerous changes (highest cancer risk)
Symptoms
Barrett’s esophagus itself has no symptoms, but patients usually have:
- Chronic heartburn & regurgitation (from underlying GERD)
- Difficulty swallowing (dysphagia)
- Chest pain (less common)
- Unexplained weight loss (if cancer develops)
Alarm Symptoms (Possible Cancer):
- Persistent vomiting
- Blood in vomit/stool
- Severe pain when swallowing
Diagnosis
- Upper endoscopy (EGD) – Gold standard (checks for abnormal pink tissue)
- Biopsy – Confirms intestinal metaplasia & dysplasia
- Advanced imaging – Chromoendoscopy (dye) or narrow-band imaging (NBI)
- pH monitoring & manometry – If GERD symptoms are unclear
Treatment
1. Non-Dysplastic Barrett’s
- PPIs (Proton Pump Inhibitors) – Omeprazole, Pantoprazole (reduce acid)
- Lifestyle changes (weight loss, diet, no smoking/alcohol)
- Regular surveillance endoscopies (every 3-5 years)
2. Low-Grade Dysplasia
- Stronger acid suppression (high-dose PPIs)
- Ablation therapy – Radiofrequency ablation (RFA) or cryotherapy
- More frequent monitoring (every 6-12 months)
3. High-Grade Dysplasia/Early Cancer
- Endoscopic resection (EMR/ESD) – Removes abnormal tissue
- Ablation therapy (RFA, cryo, or photodynamic therapy)
- Surgery (esophagectomy) – If cancer invades deeper layers
Prevention
✔ Control GERD aggressively (PPIs + lifestyle changes)
✔ Lose weight if obese
✔ Quit smoking & limit alcohol
✔ Diet rich in fruits/vegetables (antioxidants may help)
When to See a Doctor
If you have chronic GERD (≥5 years), get screened if:
- Weekly heartburn/regurgitation
- Multiple risk factors (male, white, obese, smoker)
Emergency visit if:
- Black stools/vomiting blood
- Sudden inability to swallow
- Severe chest pain
How to Avoid Barrett’s Esophagus
- Treat GERD early (don’t ignore chronic reflux)
- Sleep with head elevated
- Avoid late-night meals
- Choose GERD-friendly foods (low-acid, non-spicy)
Final Note:
While only 5-10% of GERD patients develop Barrett’s, early detection prevents cancer. If you’re high-risk, ask about screening endoscopy.






