
Forearm Fractures: A Comprehensive Guide
What it is:
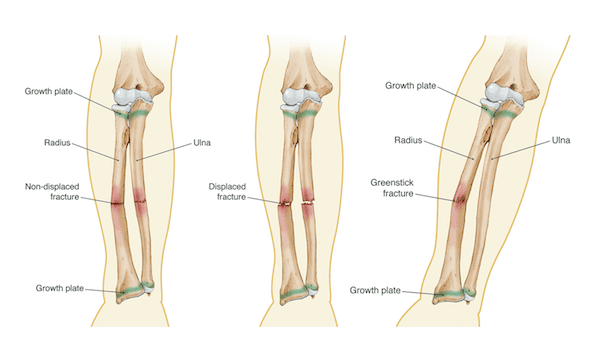
A forearm fracture is a break in one or both of the bones in the forearm: the radius and the ulna. These two bones run parallel from the elbow to the wrist. The radius is on the thumb side, and the ulna is on the pinky side. Forearm fractures are common in both children and adults and can range from a simple, isolated break to a complex injury involving both bones and the wrist or elbow joints.
Types:
Forearm fractures are classified by the bone involved, the location of the break, and the pattern of the fracture.
- Isolated Ulnar Shaft Fracture: Often called a “nightstick fracture,” as it can occur from a direct blow to the forearm, such as raising an arm in defense.
- Isolated Radial Shaft Fracture: A break in the radius alone.
- Both-Bone Forearm Fracture: A break of both the radius and ulna shafts. This is often unstable and frequently requires surgery in adults.
- Distal Radius Fracture: The most common type of forearm fracture. This is a break of the radius near the wrist, often called a “wrist fracture” or a “Colles’ fracture” when specific displacement occurs. It typically results from a fall onto an outstretched hand (FOOSH injury).
- Monteggia Fracture: A fracture of the proximal ulna (near the elbow) combined with a dislocation of the radial head (the top of the radius at the elbow).
- Galeazzi Fracture: A fracture of the radial shaft (often towards the middle or distal third) combined with a dislocation of the ulna at the wrist joint.
Symptoms:
- Immediate, severe pain that worsens with movement.
- Visible deformity or bending of the forearm.
- Significant swelling and bruising.
- Tenderness to touch directly over the break.
- Inability to rotate the forearm (turn palm up to palm down).
- Numbness or tingling in the hand or fingers (a potential sign of nerve injury).
Diagnosis:
- Physical Examination: A doctor will check for deformity, swelling, and open wounds. A critical neurovascular exam is performed to assess nerve and blood vessel function in the hand and fingers.
- X-rays: The standard diagnostic tool. X-rays are taken of the forearm, and often including the wrist and elbow, to rule out associated dislocations (like Monteggia/Galeazzi injuries).
- CT Scan: Occasionally used for complex intra-articular fractures (where the break extends into the wrist or elbow joint) to better visualize the fracture pattern for surgical planning.
Prevention:
- Fall Prevention: Using safety measures for the elderly (removing tripping hazards, improving lighting) and wearing appropriate footwear.
- Protective Gear: Using wrist guards during high-risk activities like skating, skateboarding, and contact sports.
- Bone Health: Maintaining a diet rich in calcium and Vitamin D to prevent osteoporosis.
Treatment:
Treatment depends heavily on the type of fracture, its alignment (displacement), and the patient’s age.
- Non-Surgical Treatment: Used for non-displaced or minimally displaced fractures that are stable.
- Casting: A long-arm cast is applied to immobilize the elbow and wrist. It is typically worn for 4-6 weeks.
- Closed Reduction: For some displaced fractures, a doctor can manually realign the bone fragments without surgery before applying a cast.
- Surgical Treatment: Required for unstable, displaced, or open fractures.
- Indications: Significant displacement, both-bone fractures, open fractures, fractures that involve a joint, and failed closed reduction.
Types of Surgeries:
- Open Reduction and Internal Fixation (ORIF): This is the most common procedure.
- Plates and Screws: A metal plate is contoured to the bone and secured with screws to hold the fragments in precise alignment. This is the standard for adult forearm fractures.
- Intramedullary Nailing: A metal rod is inserted down the center (canal) of the bone. This is used more frequently in children but can be an option for certain adult fractures.
- External Fixation: A temporary frame outside the body with pins that go into the bone above and below the fracture. Used for severe open fractures with significant soft tissue damage or contamination.
Prognosis:
- Non-Surgical: With proper casting and follow-up, most non-displaced fractures heal well with excellent return of function after a period of physical therapy.
- Surgical: Modern surgical techniques have excellent outcomes. The goal is to restore normal anatomy, allowing for early motion and minimizing stiffness. Full recovery of strength and motion can take several months.
- Potential Complications: Include malunion (healing in a bad position), nonunion (failure to heal), infection, nerve or blood vessel damage, and compartment syndrome (a medical emergency – see below).
Warning Signs & When to See a Doctor:
Seek immediate medical attention for any forearm injury that causes severe pain, deformity, or an inability to move the arm or wrist.
Go to the Emergency Room immediately if you experience any of the following after an injury:
- Signs of Compartment Syndrome: A medical emergency characterized by severe, unrelenting pain that is disproportionate to the injury, pain that worsens with stretching the fingers, extreme tightness and swelling of the forearm, and numbness or tingling. This requires urgent surgical intervention.
- An open fracture (bone piercing the skin).
- Numbness, tingling, or coldness in the hand or fingers.
- Fingers that are pale or blue.






